Black Shadow: A Multi-Channel Sleep Study Device
 Hypnagogia Blog
Hypnagogia Blog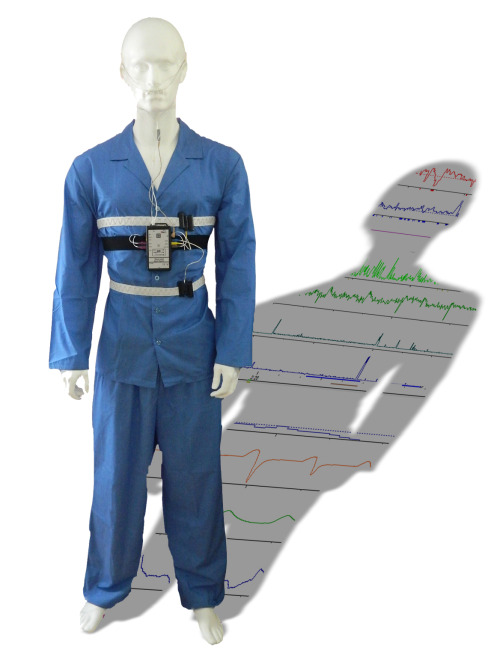
In my experiments so far I've only looked at a few "channels" of data such as airflow, blood oxygen levels and sleep stage, but when you have a full sleep study in a hospital or sleep-lab many more channels are monitored, all of which provide insights into the cause of your sleep problem.
I've recently been using a hospital-grade multi-channel sleep study device that is new to the market. It's designed to be used at home or in a sleep lab / hospital. I've been using it at home. It's called the Black Shadow and it's made here in the UK by Stowood Scientific Instruments.
The Black Shadow is capable of monitoring:
- Nasal Airflow (via a nasal cannula)
- Oral & Nasal Airflow (via a thermal sensor)
- Respiratory effort (ie breathing movements) (via 2 inductance belts)
- Pulse oximetry
- Pulse rate (via pulse oximetry)
- Plethysmograph (pulse profile)
- Sound recording and snore detection (from a small microphone on the cannula)
- Actigraphy body movement
- Body position: Left, right, prone, supine & upright
- ECG (one channel)
- Separate leg movements (via EMG or movement sensors)
- Event marker (via a patient activated button)
The system also has provision for auxiliary inputs (4). It also has provision for ECG/ EEG/ EOG/ EMG data (via an additional unit).
The prospect of having all the data available in an automated unit really intrigued me. In subsequent blog-posts I'll show how I've used the Black Shadow to verify some of my previous experiments and create some new ones, but this post is really going to be an introduction to some of the things that the Black Shadow has revealed about my sleep.
In many sleep labs and hospitals, you are connected to several bedside monitors by long wires allowing you to move in bed, but making it hard if you need to get up in the night to use the bathroom. The Black Shadow overcomes this by being wearable, so once you're connected, you are free to move around should you need to.
;)
I've no intention of posting a photo of me in pyjamas wearing the device on the internet, so I fitted it to a mannequin to illustrate how it's worn.
The next few photos illustrate some of the sensors in a bit more detail (click for larger images).
;)
Under the shirt the mannequin is wearing three adhesive electrodes which are used to record ECG data.
;)
The microphone and thermal sensor fix to the nasal cannula, which is then worn around the ears:
;)
Heel / Ankle straps are also worn to detect leg movements in the night:
Also an oximeter sensor is worn on the finger which connects via a long lead to the top of the central unit. It's a flexible probe and actually a lot more comfortable than the plastic "crocodile-type" probes that I'm used to. My mannequin's hands are a bit like mittens, so I haven't fitted the oximeter probe to him.
I decided to start from scratch and take a baseline recording of my sleep (no vitamins, no supplements, no Rematee and no alcohol). After connecting myself to the various sensors I pressed the button on the front of the unit, waited for the recording light to flash and then went off to sleep.
Configuration
The Black Shadow is Bluetooth capable, which allows you to configure the device wirelessly, and to see live data via bluetooth at the beginning of the night in order to check that all the channels are configured correctly. So after pairing with my laptop, and checking that everything was fine, I was ready to sleep.
Analysing the Data
;)
Not only was there a lot more data than I'd had access to before, but I was able to manipulate it and interrogate it in ways that I've never been able to do previously.
Once downloaded, I was able to see a graph of all the channels on one page along with some additional channels derived from the data: "Pulse Transit Time" (an indicator of intrathoracic pressure and an indicator of autonomic arousals in sleep), "R-R interval" and "Flatness".
The channels are able to be moved up and down the screen so that you can, for example, put the SPO2 (oxygenation) on top of the airflow channel, making it easy to spot correlations.
The software will perform an analysis on the data (using customisable criteria) and display it in a multi-page report. Once the data has been analysed, markers appear on the graphs showing events such as apnoeas, hypopneas, pulse rate changes, oxygen desaturations, snores etc.
Zooming in on an event allows you to verify it, and if necessary disregard it.
Positional Data
As expected, it was easy to spot that I did indeed have respiratory events through the night. Once analysed, my AHI was calculated to be 7.24 which agrees nicely with my previous 5-day mean score of 7
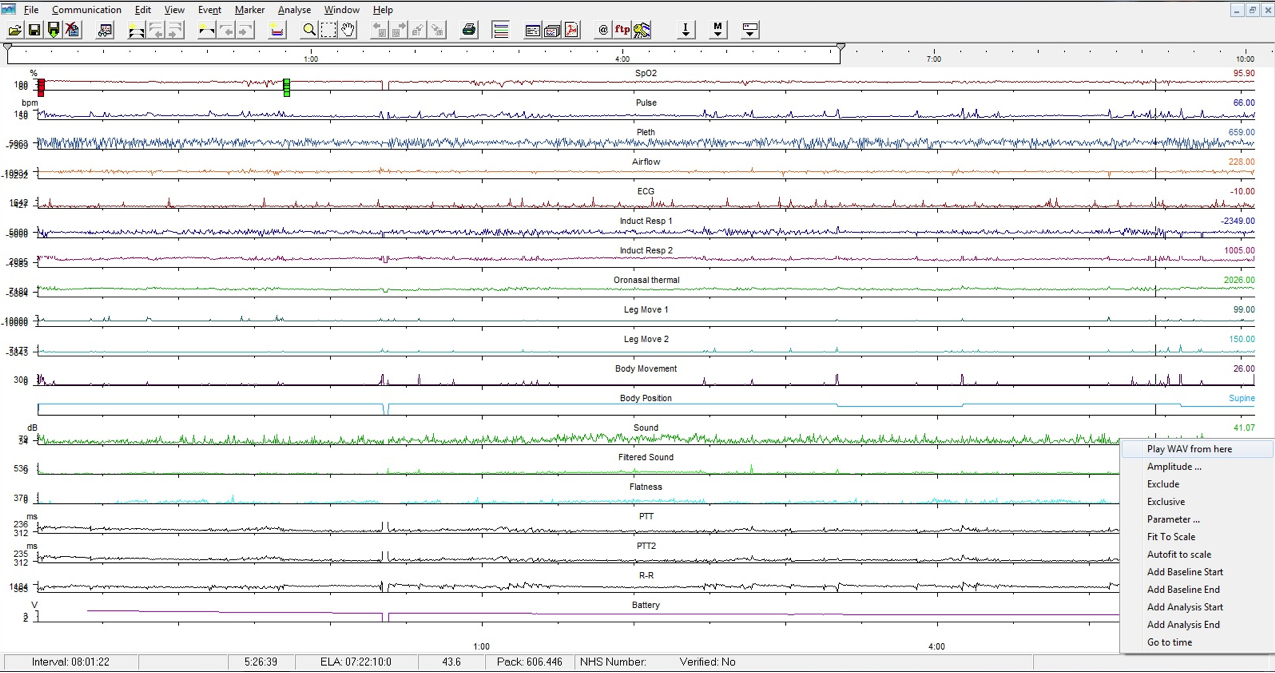
Comparing selected channels with the body-position channel, it was also easy to see that the vast majority of my respiratory events occurred while I was sleeping on my back. (Click for larger image).
;) The body position channel (3rd down) shows the first half of the screen with me on my back turning onto my right side for the second half.
The body position channel (3rd down) shows the first half of the screen with me on my back turning onto my right side for the second half.
Comparing the supine to side-sleeping data it is clear that (From the top down):
- My SPO2 (oxygen saturations) are higher and stable with side sleeping
- My pulse is lower and stable
- Change in body position from Supine to Right
- My snoring stops (filtered sound channel)
- My oral/nasal airflow is stable
- My leg isn't twitching
- My body movement is greatly reduced
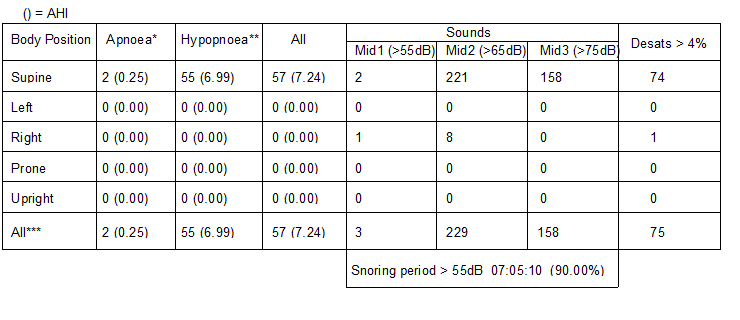
The improvement is revealed in a table in the report:
It's possible to exclude periods of data from the analysis by highlighting them; so for example, by only looking at the periods when I slept in a supine position (on my back) I could see how my AHI was if I only slept on my back.
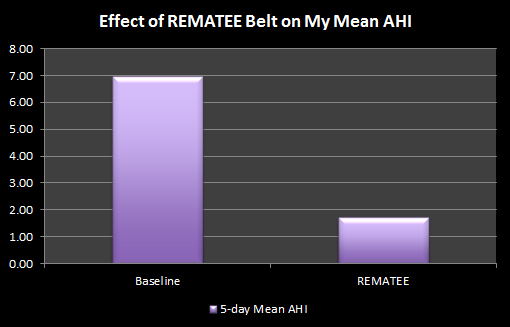
All of this is a great indicator that positional therapy such as the Rematee would help my sleep problem.
Obstructive vs Central Apnoeas
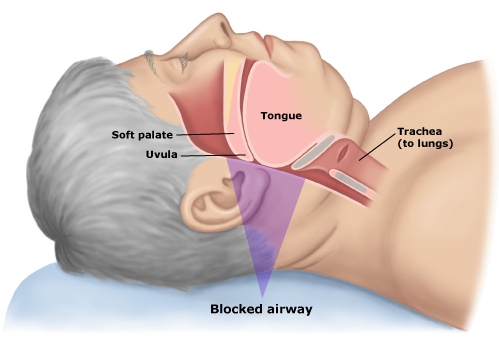
The two respiratory effort channels allowed me to see whether my apnoeas were obstructive or central in nature. Obstructive apnoeas are where the body still tries to breathe (ie the intercostal and diaphragm muscles still move as normal) but the airway is obstructed, rendering the effort useless. Central apnoeas are where the brain doesn't signal the muscles to breathe, or the signal is blocked for some reason.
Each respiratory effort graph relates to one of the inductance belts that are worn around the chest and stomach. The graph therefore shows the chest and stomach movements, and hence if an effort to breath was made how strong it was in relation to other breaths.
My graph showed that I still attempted to breathe and yet no airflow was recorded, this makes my apnoeas obstructive in nature. (Click for larger version)
;)
Audio Recording & Snore Detection
The Black Shadow records sounds continuously through the night, so unlike my attempts with a voice-activated dictaphone, you are able to hear sounds leading up to an event rather than just a second or so after the event itself.
Because the microphone is calibrated, the sound channel is graphed according to sound amplitude in dB. The software also creates a second sound-channel of sound that is filtered to highlight snoring. The detected snores are then marked automatically, making it easy to click on the graph and actually hear the snore. Listening to sound can be done at any point of the night, not just snores, so it's possible to hear sleep-talking and other noises.
I'd like to say that I sleep silently, and that the Black Shadow didn't detect any snoring from me, but that would of course be a lie because I snored a lot. The report (above) showed that I snored at a level of above 55dB for 90% of the night! 158 snores were louder than 75dB, which is roughly the noise level generated by a lawnmower!
This is a screenshot of 23 seconds of my sleep. Four snores are shown which were detected and marked automatically, these correspond to the snores that have been isolated on the filtered channel. What I find interesting about this screenshot is that the vibrations caused by my snoring are visible on the airflow channel (top - orange line).
(Click for a larger image)
;)
Again, I was able to see that most of my snoring took place while I slept on my back.
Leg Movements
When I took a look at the leg movement data I saw something that surprised me.
Like most people, as I drift off to sleep, I twitch a bit. If I'm laying on my back I know that my left leg is prone to having the odd twitch (since I injured a disc at L5 in my spine), and this also happens when I'm sitting using my computer late at night, but I didn't suspect it happened when I was asleep. Looking back, I probably should have done.
Sometimes arousals from respiratory events will cause a body or leg movement, but I was seeing these twitches in periods of sleep that were free of respiratory events.
This is what I saw when I looked at a 12 minute section of my data (click for larger image):
;)
At 1:15 am my left leg (leg 1) started to twitch slightly, and as you can see the amplitude increased almost with each subsequent movement over the next 4 minutes. This then caused me to turn from my back onto my left side (shown by the Body Position channel in blue). This happened several times a night, in all sleeping positions and on more than one night. Although I haven't been able to eliminate them, maybe this is an indication of why the Vitamins and Minerals improved my sleep as Iron is thought to be beneficial to Periodic Limb Movements.
Those legs movements and the subsequent turning over could be a problem if it happened often enough because it is yet another thing that can cause a sleeper to awaken briefly. These small awakenings are called micro-awakenings (or micro-arousals). The higher the number of these there are in a given night, the more your sleep is disrupted and the greater the likelihood of waking in the morning still feeling tired. If I want to improve my sleep further then these are the sort of things that I need to be aware of.
Pulse Rate Increases
The Visi-Download software also shows other arousals which are calculated from my heart-rate data.
This section of my sleep shows how a cluster of respiratory events (marked by the blocks under the airflow line) affected my oxygen saturations (top red line). If you look at the other data shown in line with those events you'll see that not only was my heart rate affected, but also my Pulse Transit Time - a very good indicator that I was continuously being woken (brief)y by my respiratory disturbances, causing fragmented sleep.
;)
The Pulse Plethysmograph also shows changes, even on this timescale because the arousals went on for a prolonged period of time. Shorter micro-arousals are able to be seen using the PTT and Pleth channels when looking at a smaller timeframe.
Event Marker
Pressing this button during recording causes a marker to be inserted into the data. This could be for any event, such as being woken, waking from a nightmare, feeling unable to breathe, or even (as I plan to use it) for marking lucid dreams and sleep paralysis.
The Black Shadow opens up many additional ways for me to explore and hopefully improve my sleep and I'm looking forward to experimenting further with it.
Additional Links
Non-invasive Monitoring of Vital Signs Utilising Pulse Wave Transit Time
Obstructive Apneic Events Induce Alpha-receptor Mediated Digital Vasoconstriction - Zou et al


;)


;){kind=link}
;){kind=link}