Sleeping Position - Supine AHI: A Baseline Measurement
 Hypnagogia Blog
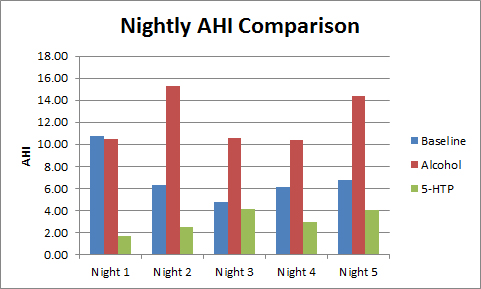
Hypnagogia BlogLooking at my previous data for my 5-day mean AHI, you can see some variation on the day-by-day AHI measurements.
It makes sense that each night will be slightly different but I still wanted to identify and eliminate some of these variables. Now that I know that my sleep-apnoea is positional (mainly when supine) I can attribute some of the night-by-night changes to my sleeping position.
Using the Black Shadow sleep monitor, I am able to automatically record my body position during the night. This is a recording of my sleep position for a single night.
;) AHI = 9.30
AHI = 9.30
As you can see from the above chart I spent a fair chunk of the night on either my right or left side. Those short spells on my back are when my sleep apnoea kicks in (or the snoring is so loud that it wakes me up). The reason that they are only short spells is that the apnoeas briefly wake me causing me to move onto my side for an hour or so before ending up on my back again (and beginning the cycle again). Towards the end of the sleep I remained on my back despite the apnoeas causing repeated micro awakenings (micro-arousals).
Prior to having access to accurate sleep position data I was aware that sleeping position (and other variables) could affect my AHI, so in my previous experiments I tried to eliminate its effects by recording 5 consecutive nights and calculating a mean AHI. Solely recording one night could have given a falsely low AHI because if by sheer chance I managed to spend the majority of the night on my side then my AHI would have been lower. This lower AHI would actually be masking my problem.
A recent paper by Sunnergren, Broström & Svanborg shows that "Position–dependent obstructive sleep apnea (POSA) was common both in subjects that by American Academy of Sleep Medicine classification had obstructive sleep apnea as well as those without. The severity of obstructive sleep apnea, as defined by American Academy of Sleep Medicine, could be dependent on supine time in a substantial amount of subjects".
This hints that people are slipping through the net and missing out on a diagnosis and treatment.
It is for this reason that a sleep-study conducted in a sleep-lab or a hospital tries to have at least part of the night recorded with the patient sleeping on their back (and with some REM sleep too).
The Visi-Download software allows me to include/exclude portions of the night based upon custom criteria, so I manually selected only the times that I slept on my back and re-ran the analysis.
Using this method, my Supine AHI for the 9.30 night shown above was actually 12.73, for which I snored at a level of above 55db for 95.5% of the time! For the record, my lowest oxygen desaturation took me to 79%.
Using this method, my supine AHI is more stable, (although not completely the same every night) this demonstrates that this is actually a more consistent method of calculating my night-time AHI, although for others with non positional apnoea it may well be a different story.
I plan to carry out some further monitoring without the Rematee, so this is the method I will use to ensure a fairer compaison between nights.