Actigraphy: Only Part of the Story...
 Hypnagogia Blog
Hypnagogia BlogActigraphy, or the monitoring and charting of the movement that we make, is an established means of monitoring sleep, albeit not a very detailed one.
The patient wears a movement monitor(s), the data from which is essentially processed as "not moving = asleep" and "moving = awake". As you can see, this can only really tell us the two states and not provide more accurate sleep stage information.
Actigraphy is not a substitute for a full sleep study, however the data it provides can be used to augment a sleep study.
There are many consumer actigraphy devices on the market today, and also many intended for professional use. I am only concentrating on the consumer devices. The professional devices are a lot more sophisticated.
A few months ago I tried out a couple of the consumer devices myself, and pretty much dismissed them as I found that they didn't really add anything to my existing set-up consisting of nasal airflow, oximetry, capnography, IR camera and the Zeo.
First let's take a look at the devices and the data they provide:

The first device is the "Wakemate". This consists of a small circuit board that fits inside a wrist-worn sweatband.
The on-off switch protrudes directly from the circuit board, which had me worrying that it would soon break after repeated use, however it seemed secure enough once tucked inside the padded band.
Once paired with your smart-phone, the device uploads its data via bluetooth.

The second device is the "Lark".
This is similar to the Wakemate, although it felt sturdier and had a nice charger dock with it.
The electronics are encased in a sealed unit which is then inserted into the wristband.
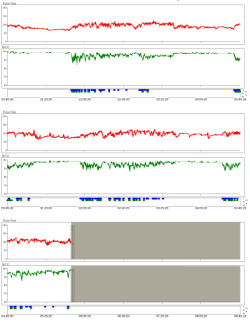
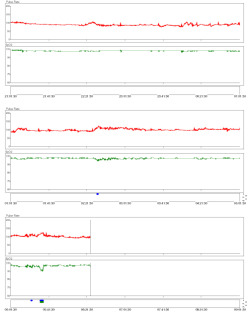
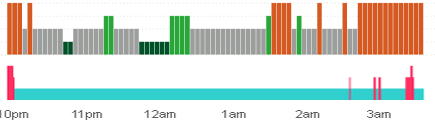
To give a fair test to these gadgets, I wore them both on the same night, both on my non-dominant wrist. Once I'd downloaded the data I was able to find a chart of time vs movement. Both charts aligned well:
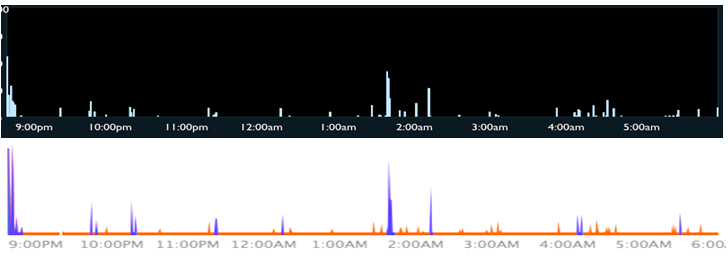
(Wakemate - top. Lark - bottom)
The Lark's graph is more detailed than that of the Wakemate, and shows some analysis has already taken place on the data. It highlights large movements blue signifying periods of wakefulness and leaves smaller movement orange.
More data is available from both devices, such as total time awake, total time asleep, time in bed etc.
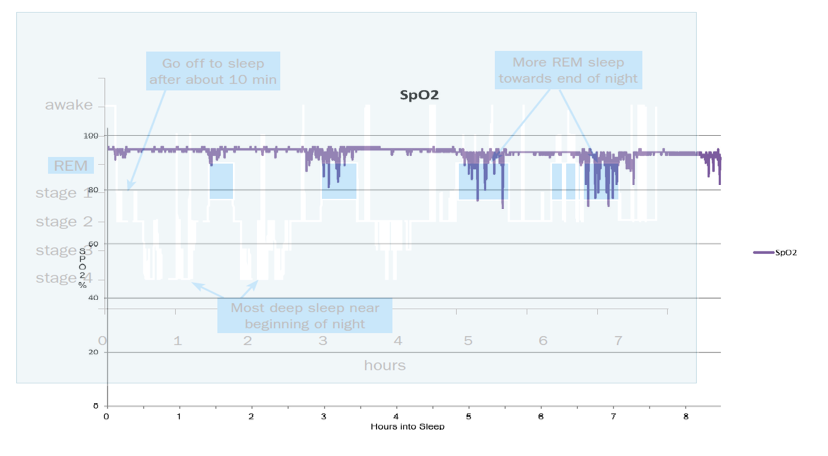
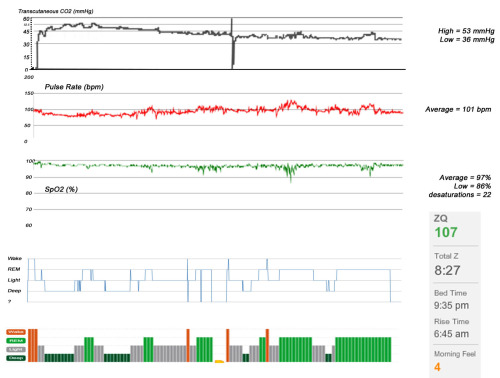
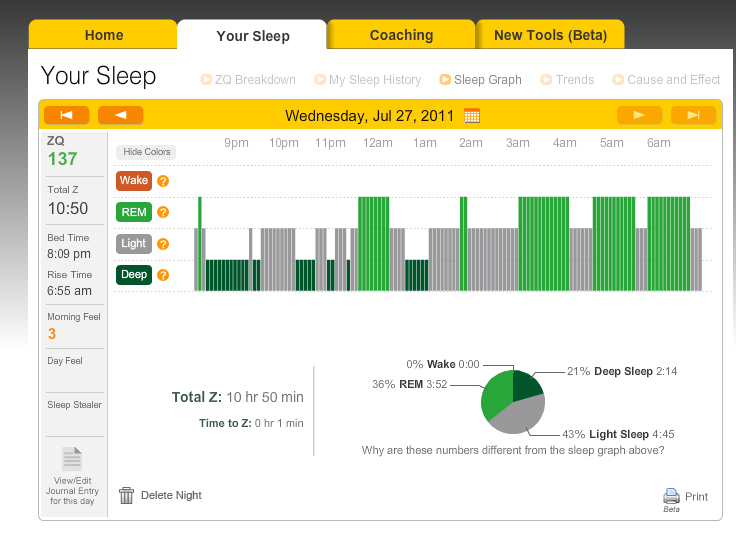
I then compared the above graphs with the Zeo hypnogram from the same night...
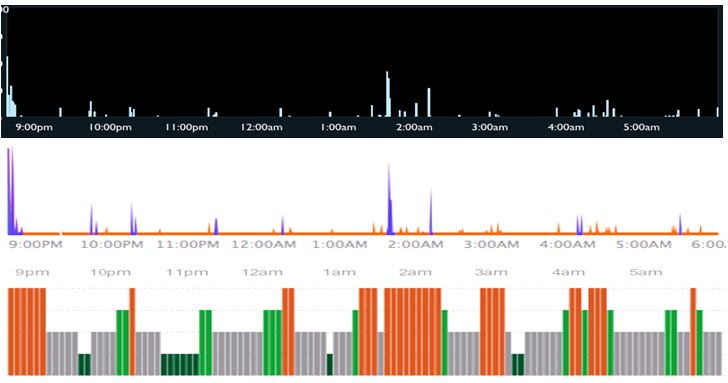
By doing this some of the limitations of actigraphy become clear. I was actually awake for an hour between 1:15am and around 2:15am. During this time I was lying still, hoping to fall asleep again. The actigraphy-based devices interpret this period of stillness as sleep, albeit with some movement. Being still does not equate to being asleep. Consequently, if a partner is moving around in the same bed as you, it is possible that the actigraphy would detect their movement.
However, it was good to have my broken REM (around 4am) confirmed by the actigraphy devices. At this time I was suspecting that the Zeo was detecting some of my REM as wakefuness (a suspicion that I later ruled out). During normal REM sleep muscle atonia prevents us from moving, so seeing that I actually moved during REM added to the growing evidence that I really did wake during REM sleep.
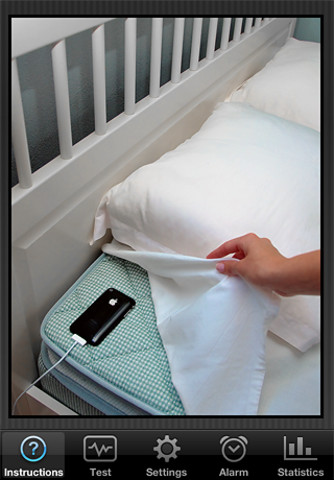
Whilst looking into actigraphy, I also found a popular iPhone app that makes use of the accelerometer in the phone. It's called Sleep Cycle.
The phone is placed at the top of your bed, near your head, it then monitors your movement (based on how the bed moves) in the night.
It's actually very simple, but I found that it was surprisingly accurate when compared to the Zeo. It correctly identified two periods of being awake and one period of deep sleep. I suspect in a healthy sleeper, it would confuse REM sleep and deep sleep.
I have also used the AxBo "SleepPhase" alarm clock. This is a clock that comes with two wristbands which wirelessly communicate with the clock. Each wristband contains a sturdy sealed module that detects movement. The intention is that two people can use this clock.
I purchased the AxBo before I had any other consumer devices. I still had the oximeter and the capnograph, but no Zeo and none of the actigraphy devices mentioned in this blog-post.
However, after purchasing the clock and using it for one night, I realised that it doesn't actually show sleep stages. I probably should have realised beforehand.
The sensors are actually very sensitive, and show more movement information than anything I've previously discussed here. They can actually show which axis the movement takes place along. However, after a couple of nights of wearing the band and looking at my movement data I thought "Okay, but so what?". I wasn't actually sure where to go from there as I wasn't interested in the clock's ability to wake me up at an optimal time, more in its ability to chart my sleep.
A device for sleep and wake?
 As part of a health kick (and weight loss), I have been using a device called "FitBit". It looks like a very slick pedometer, but it is acutally a lot more sensitive. It uses an accelerometer to determine steps taken in day, how many flights of stairs you climb, how many calories burned, and sleep-actigraphy similar to the devices mentioned above.
As part of a health kick (and weight loss), I have been using a device called "FitBit". It looks like a very slick pedometer, but it is acutally a lot more sensitive. It uses an accelerometer to determine steps taken in day, how many flights of stairs you climb, how many calories burned, and sleep-actigraphy similar to the devices mentioned above.
The difference between this and a standard pedometer is that this can show you, in graph form, when the activity occurred during the day.
The bonus with the FitBit is that the "FitBit Dashboard" lets you link your data with other "Quantified Self" devices such as the Withings bathroom scales, which in turn lets you link your data with your Zeo ZQ.
This all adds up to a feeling of being part of a bigger programme, a programme that encourages you to look at all aspects of your health see the effect that lifestyle changes have on your data (and on you). You can actually quantify your exercise, which in turn reveals a greater weight-loss which hopefully will have an effect on my sleep quality, which will be seen in the ZQ.
Anyway, I've lost 9lb so far and I plan to carry on until I get down to my target weight and then I'll blog the combined results.
Quantifying the exercise that I do in terms of steps taken, flights climbed and calories used should allow me to see a correlation between FitBit exercise and Zeo deep sleep, maybe a correlation with sleep and a quantified "power-down hour" in the evening; who knows, it may even reveal a REM correlation too.
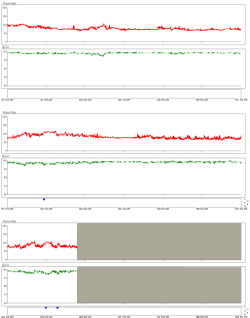
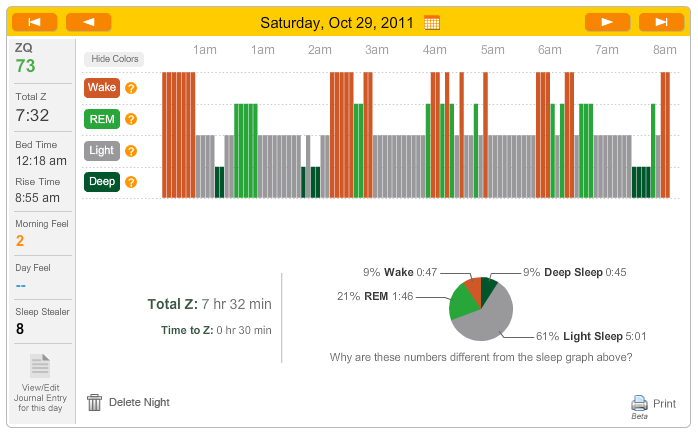
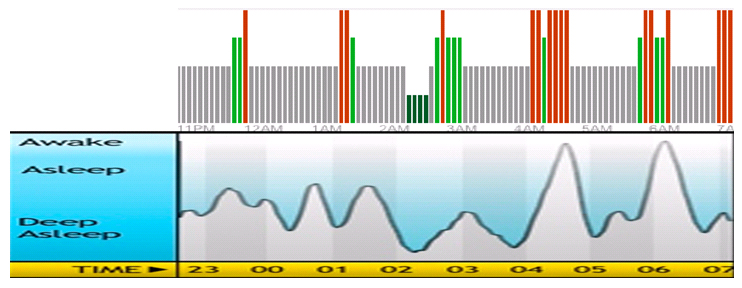
How did FitBit do when compared to Zeo for sleep analysis?
Again, it compared well, with the exception mentioned above (that being still in bed does not equate with being asleep), and to be fair, the Zeo 30 second data does show me drifting into and out of sleep at a couple of points in the large period of wakefulness at the end before I eventually gave up and got out of bed, but for the most part I was awake and just being still.
However, none of the actigraphy devices show sleep-stage data, and (as I'm learning from the fascinating "Quantified Self" movement) more data means a greater ability to "hack" yourself or to help yourself.
By using actigraphy as the sole gauge of good sleep you are blind sleep stage data. Having access to my sleep stage data allows me to target specific stages that I think need attention: If your slow-wave-sleep (deep) is too low then you can exercise to increase it. If your REM is broken or too low then you can try supplements and mental exercises to put it right. This is not possible if you can only tell that you were moving when you were supposed to be asleep.
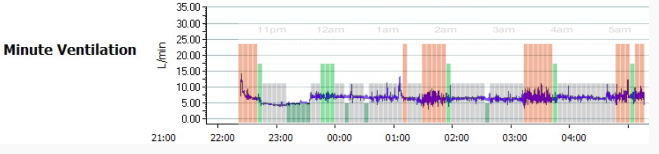
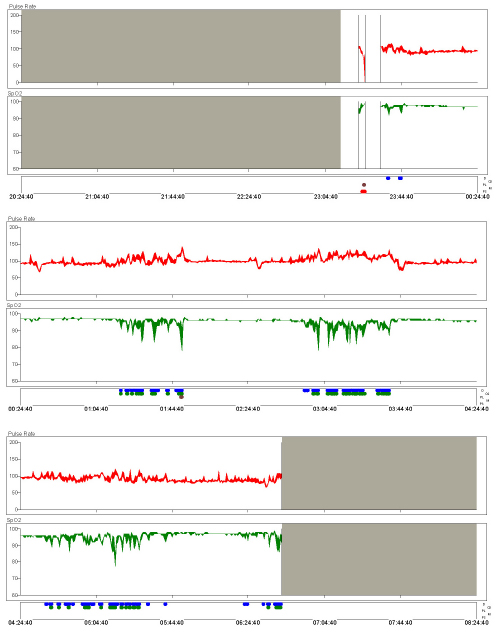
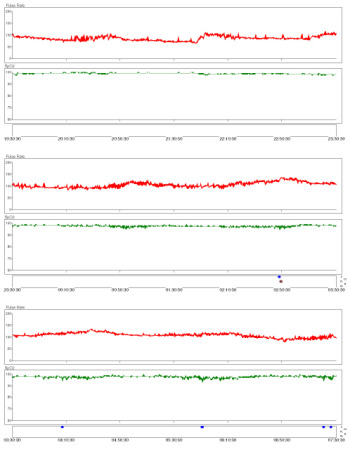
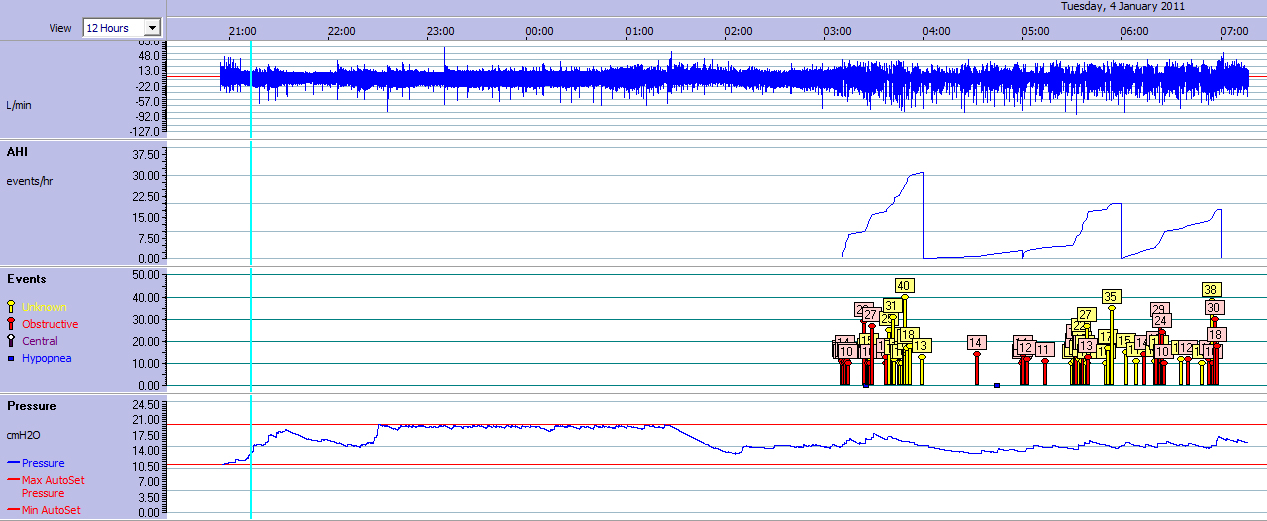
Having easy access to my sleep stage data set me on the road to investigating why my REM sleep was broken. I was easily able to correlate my drop in oxygen levels to REM sleep using a cheap pulse-oximeter, and from there, with the addition of another channel - airflow, discovered that REM-related apnoeas were the cause. From there with the addition of another channel (motion activated IR camera) I was able to add "positional" and "obstructive" to that diagnosis. Giving me the full diagnosis of "Mild REM-related positional obstructive sleep apnoea".
With a correct diagnosis, I was then in a better position able to properly assess treatments (more of those in a later blog).
This would not have been possible had I only known that I moved during my sleep as the correlation with REM would not have been detectable, although, to be fair,I could have gone onto diagnose apneoa without sleep stage data, it would have not given me the full picture. In fact looking at my sleep using only actigraphy (when I only had the AxBo), made me pretty much give up after a couple of nights. Nothing made me want to look into my sleep further until I had the Zeo and Oximetry data.
I continue to use the FitBit during the day, but I eventually consigned the other sleep-actigraphy gadgets to the bottom drawer until I realised that by using these devices slightly differently that I could use them to add additional channels to my setup, in theory anyway...
A cause of poor sleep is Periodic Limb Movement Disorder, in which the sleeper's legs twitch and move involuntarily during the night, causing them to wake up, or partially wake up (micro-arousal), both of which lead to disturbed sleep.
By fixing the actigraphy devices to the sleeper's ankles it would be possible to detect this. It might even be possible to detect the leg movements as a cause of waking up, rather than as a consequence of it if the devices could be accurately synchronised. The only thing that concerns me about this is that the timescale on the axis of the movement graphs may not be detailed enough to show the movements occuring before an awakening. Oddly, I think the Axbo would be best suited to this, as the software allows the most flexibility in analysing the data. However, this will have to remain a theoretical test as I don't have an issue with PLMD.
(All device photos are from product websites unless indicated)